
In my previous post, I estimated that 47% of pregnancies are unintended, and of these, 43% occur in countries where abortion is illegal or severely restricted. In countries where abortion is widely available, 71% of unintended pregnancies are aborted compared to 46% in countries with severe restrictions.
The World Health Organization (WHO) estimates that around one-third of the 23 million induced abortions carried out each year in countries where abortion is severely restricted are performed under the least safe conditions, by untrained persons using dangerous and invasive methods. Safe abortion is an essential health care service. It is a simple intervention that can be effectively managed by a wide range of health workers using medication or a surgical procedure. In the first 12 weeks of pregnancy, a medical abortion can also be safely self-managed by the pregnant person at home.
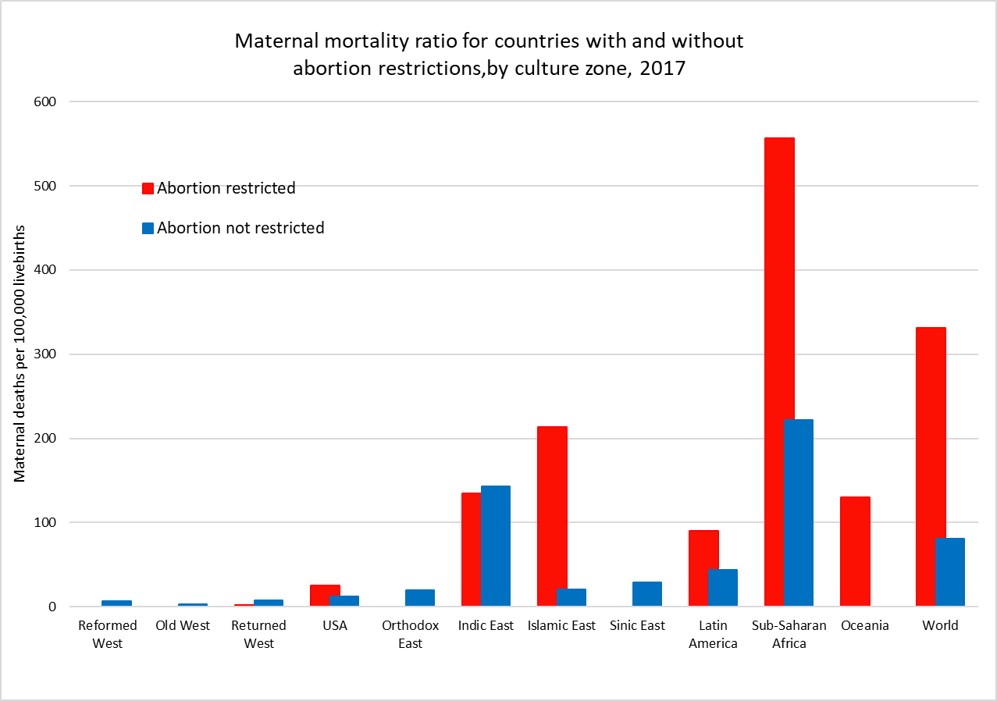
Maternal mortality is defined as death while pregnant or within 42 days of the end of pregnancy from any cause related to or aggravated by the pregnancy or its management. The plot above shows the average maternal mortality ratio (MMR) per 1,000 live births for countries (and US states) grouped by access to abortion and culture zone for the year 2017 (see here for more details).
While countries that restrict abortion have higher MMRs than those that don’t for most of the culture zones, we cannot conclude that abortion restriction per se is responsible for the difference. Abortion restriction is also correlated with other determinants of higher MMR such as lower average income per capita, less access to health care, and higher levels of discrimination against women.
The global MMR has declined from 345 per 100,000 livebirths in 2000 to 212 per 100,000 livebirths in 2017, a 40% decrease in 17 years. There have been substantial declines in MMR in every culture zone except for the Reformed West and Old West where MMR rates were already very low in 2000 and in the USA where rates have risen substantially during the 21st century.
The plot below takes a closer look at MMR trends in the USA, the Reformed and Old West, the Returned West and the Orthodox East. The latter two culture zones include the former Soviet bloc countries. With the exception of Poland in the Returned West, all these culture zones except the USA do not restrict access to abortion services and allow abortion on request or in some countries on “economic and social grounds”.
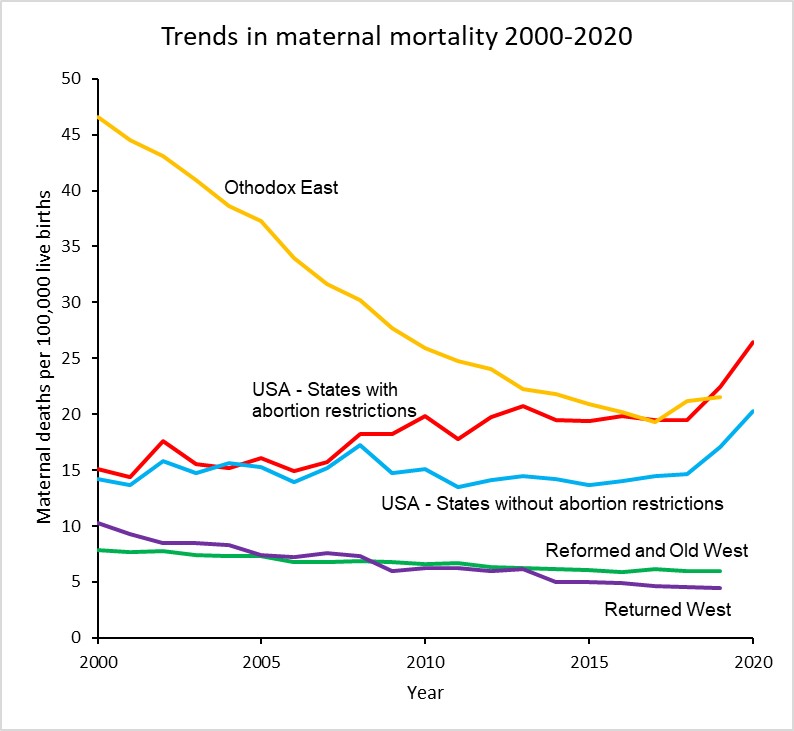
The maternal mortality ratio for the USA has increased from around 15 per 100,000 livebirths in 2000 to 23.8 in 2020, a 62% increase. Abortion rates in States which now restrict abortion were similar to those in states which don’t until 2008 and afterwards diverged substantially. The rate for states with restrictions was 26.4 in 2020, 30% higher than the MMR of 20.2 for states without restrictions.
There has been considerable controversy about the substantial increase in maternal mortality in the USA, particularly as to whether it is associated with improvements in the identification and reporting of maternal deaths. The addition of a pregnancy checkbox to death records from 2003 onwards is thought to have led to some increase in estimated MMRs in the early 2000s, but several studies have also identified that increasing restrictions on the general availability of reproductive health services have played a major role, particularly in states restricting access to abortion.
Hawkins et al (2019) found that a 20% reduction in the numbers of Planned Parenthood clinics resulted in an 8% increase in maternal mortality and states that enacted legislation to restrict abortions based on gestational age increased the maternal mortality rate by 38%.
A 2020 study by the Commonwealth Fund compared maternity care in the USA with 10 other developed countries and found that the USA has the highest maternal mortality among developed countries and that there is an overall shortage of maternity care providers (obstetrician-gynecologists and midwives). The USA has 12 to 15 providers per 1,000 livebirths, and all the other developed countries have a supply that is between two and six times greater. Although a large share of its maternal deaths occur postbirth, the U.S. is the only country not to guarantee access to provider home visits or paid parental leave in the postpartum period. In the early 2000s, WHO estimated that unsafe abortion accounted for around 13% of total global maternal deaths, then estimated to be around half a million deaths per year. A more recent study by WHO staff and academic colleagues in 2014 estimated that abortion accounted for 7.9% of maternal deaths at global level between 2003 and 2009. Recent WHO estimates for global deaths by cause do not include deaths due to induced abortion. I have elsewhere used results from the Global Burden of Disease Study 2019 to estimate very approximately the proportion of maternal deaths due to abortion and miscarriage for the period 2015-2019. These would include induced abortion deaths as well as deaths due to spontaneous abortions and miscarriages. The following plot shows the estimated average percent of maternal deaths attributed to abortion and miscarriage for countries with and without abortion restrictions in each culture zone.
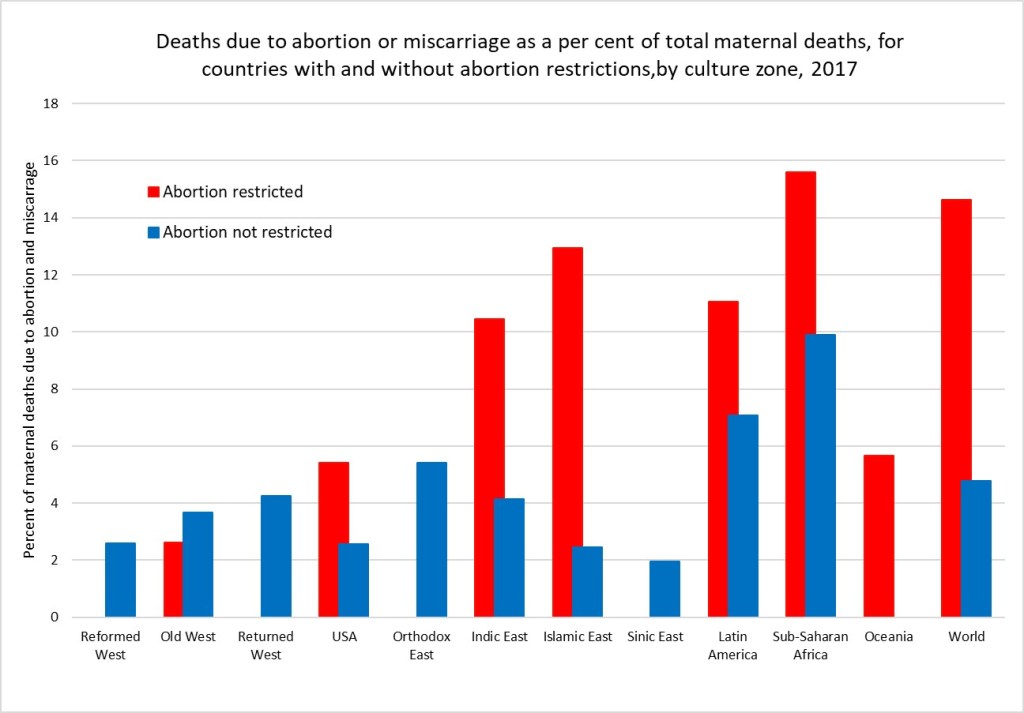
Overall, I estimate that there were 75,500 deaths globally due to abortion and miscarriage in 2017 (these include spontaneous events as well as induced abortions). Of these 70,300 were in countries with abortion restrictions. Assuming the rate in countries with unrestricted abortion relates to the spontaneous events, I have estimated that abortion restrictions resulting in unsafe abortions caused 54,350 deaths in 2017. If all abortions were safe, there would have been only 21,200 deaths globally due to spontaneous abortion and miscarriage in 2017.
Its quite possible these very back-of-the-envelope estimates are under-estimates. Classification of maternal deaths due to abortion, and more specifically unsafe abortion, is associated with a risk of misclassification. Even where induced abortion is legal, religious and cultural perceptions in many countries mean that women do not disclose abortion attempts and relatives or health-care professionals do not report deaths as such.
A medical abortion procedure uses the drugs mifepristone and misoprostol which can be taken in pill form up until the 12th week and are very safe. They require no surgery or anaesthesia. These drugs were developed in 1980 and first became available for induced abortions in France in 1987. It became available in the USA in 2000 and is on the WHO list of essential medicines. Cost and availability limits access in many parts of the developing world.
It is usually possible to carry out this procedure oneself at home. During the covid pandemic, a number of countries including the UK have made abortion accessible via an online consultation after which the pills are sent by post to the woman to take at home. The Netherlands-based charity Women on Web aims to prevent unsafe abortions by providing abortion pills to women in countries where safe abortion is available.
In December 2021, the FDA made permanent a covid-era policy allowing abortion pills to be prescribed via telehealth and distributed by mail in US states that permit it.Even before the FDA action,abortions induced by pills rose to more than 54 percent of all U.S. abortions in 2020, according to the Guttmacher Institute. Nineteen states have banned prescription of these pills via online consultation, requiring the woman visit a physician. And of course, in states which severely restrict abortion, this will require a completely unnecessary trip out of state.
Women on Web is making medical abortion available to women in the USA and elsewhere who are facing these restrictions. The cost for a woman to obtain the pills for a medical abortion is 90 Euros, or around 100 US dollars. You can donate to fund abortions for women unable to afford them here. Or to US based abortion funds here.
While legal abortions done under the guidance of a professional are the gold standard. Self-managed abortion can be safe, too, if you have the right information. But as I noted above, the banning of abortion typically goes hand-in-hand with restrictions on contraception and reproductive health services, as well as discrimination and other restrictions on women that result in higher maternal mortality rates, more femicide and abuse, less access to education and employment, and greater female poverty levels.
The removal of a basic reproductive rights for women in the USA is being driven by a minority, many of whom are fundamentalist Christians. According to a recent survey, white and Hispanic fundamentalists are the only religious group in the USA for which a majority oppose the legal availability of abortion (The Economist, May 7, 2022).
I discussed in a previous post how enforcement of social norms governing human fertility have been a major factor in pre-modern religions. For thousands of years, very high levels of child mortality and other survival pressures meant that most societies sought to ensure that women produced as many children as possible and discouraged divorce, abortion, homosexuality and contraception. Additionally sexual behaviour, particularly that of women and that not linked to reproduction, was strongly socially controlled to minimise uncertainty about paternity. Religion was the primary method of social control and pre-modern values regarding women’s rights, reproduction and sexuality are still dominant in most of the major religions, particularly fundamentalist forms. In a world facing overpopulation, global warming, habitat destruction and species extinction, it is crucial that outdated and cruel pre-modern values do not condemn women to reproductive slavery and an inability to control their own fertility, and reduce our ability to address these inter-related crises using all the tools and knowledge now available.
