In my first post on near-death experiences (NDE), I recalled two incidents where I was knocked unconscious and would never have known if I had died (which was by no means unlikely). The following two incidents are quite different. In both cases I fell off a cliff and was fully conscious till I hit the ground below.
Let me not spend my life lamenting the world’s sorrows for above in the wide sky the moon shines pure
ukiyo to mo omoi-tōsaji oshikaeshi tsuki no sumikeru hisakata no sora
— Saigyo
I came across this poem quite by accident. But it really struck home, as I’ve been spending too much time thinking about the state of the world right now. The human race appears to be quite incapable of working together to address the existential crises of the pandemic, global heating and species extinctions, and overpopulation, as well as the rejection of reason and science dramatically exacerbating these potentially soluble crises. Humans have not reacted to these crises in general by pulling together, given that collective action can indeed address and ameliorate, if not completely address, them. But ratherhave retreated back into tribes who blame the “other” for all their problems. It is indeed difficult sometimes to remember the moon shining pure in the wide sky.
Saigyō was the Buddhist name of Fujiwara no Norikiyo (1118–1190), a Japanese Buddhist monk-poet. He is regarded as one of the greatest masters of the tanka (a traditional Japanese poetic form). He influenced many later Japanese poets, particularly the haiku master Basho.
Saigyo was born into a branch of the Fujiwara clan, the most powerful family in Japan in the early 12th century. As a young man he joined the Hokumen Guards who served at the retired Emperor’s palace. Despite a seemingly assured future, he decided at the age of 23 to “turn from the world” and become a reclusive wandering Buddhist monk. He spent the rest of his life in alternating periods of travel and seclusion with occasional periodic returns to the capital at Kyoto to participate in imperial ceremonies. During this period, the second half of the 12th century, Japan was wracked by civil war
The translation of the poem above is by Meredith McKinney, who has published a selection of over 100 poems by Saigyo in the collection Gazing at the Moon: Buddhist Poems of Solitude (September 2021). The poems selected focus on Saigyo’s story of Buddhist awakening, reclusion, seeking, enlightenment and death. I can highly recommend this collection, which embodies the Japanese aesthetic of mono no aware — to be moved by sorrow in witnessing the ephemeral world.
Meredith McKinney is an award-winning translator of classical and modern Japanese literature, who lived and taught for around 20 years in Japan. She returned to Australia in 1998 and now lives near the small town of Braidwood, not far from Canberra where I lived until early 2000. I was interested to learn a little more about her, and was surprised to find out that she is the daughter of Judith Wright (1915-2000), one of Australia’s greatest poets and an activist for the environment and indigenous rights. For the last three decades of her life, Wright lived near Braidwood. She became completely deaf in 1992 after progressively losing her hearing since early adulthood.
I recently came across a headline referring to a 2016 survey in Iceland which found that 0.0% of Icelanders 25 years or younger believe God created the world. My immediate impression was that this implied a zero per cent prevalence of atheism in this age group. When I read the article, I found that the relevant question gave respondents four options: the world was created in the big bang, the world was created by God, the world was created by other means, or no opinion. Outside of countries dominated by fundamentalist religious groups, most religious people would likely choose “created in the big bang”. The survey actually found that 40.5% of respondents aged 25 years and younger said they were atheist, and 42% said they were Christians.
It is certainly the case that the prevalence of atheism is higher in younger ages in the developed countries where religiosity has been declining for decades. So I thought I would take a look at the prevalence of atheism in younger adults aged 15-34 years from the Integrated Values Surveys [1-3] that took place in the last wave, in the period 2017-2020. See my earlier posts (see here and here), which examined global, regional and country-level trends in religious belief and practice, for more details on the data and definitions of atheism and religiosity categories.
Countries with the highest prevalence of atheism and non-religion in 2017-2020
The following plot shows the prevalence of religious and irreligious adults for the 31 countries with the highest irreligious prevalence (atheists plus non-religious). China and South Korea lead these countries with irreligious prevalences over 80%, followed by Sweden, Czechia, New Zealand and Japan, with prevalences in the 70’s. In terms of atheism, there are 18 countries with prevalences over 50% in the 15-34 year age group, including Australia at 53%.
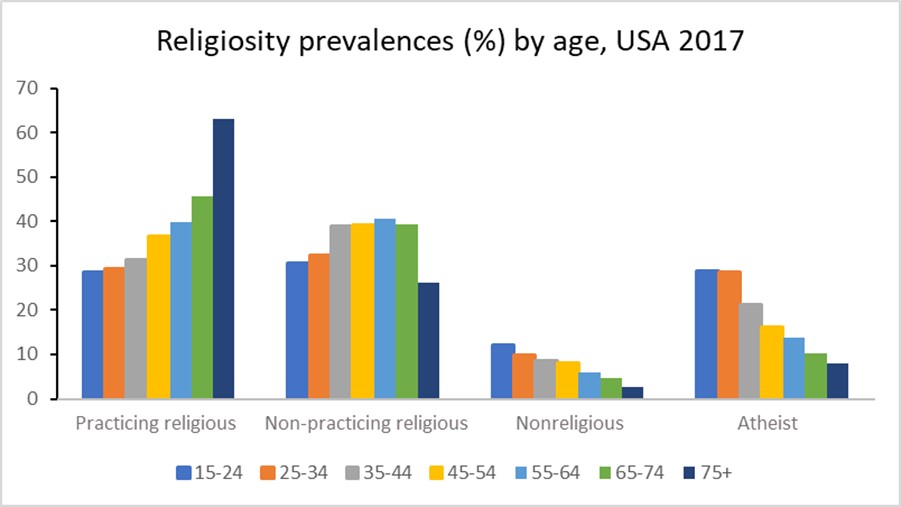
In these countries, the prevalence of practicing religious generally increases with age and the prevalence of atheists generally decreases with age. The plot for the USA 2017 survey data below illustrates this.
Are these prevalence patterns predominantly due to ageing, time period or birth cohort? Since period = birth year (cohort identifier) + age it is not possible to determine the separate effects of all three factors. Ageing as a driver of religiosity would imply that people become more religious as they get older, and this seems the least likely of the three factors to fit observed age patterns over time.
Relative contribution of cohort and period to the overall trends in religiosity
I’ve attempted to estimate the relative contributions of birth cohort and period to the evolution of religiosity in the USA using a cohort projection model. I first used the data from all waves of the US surveys to impute religiosity prevalences for years 1980, 1990, 2000, 2010, and 2020. I then projected religiosity prevalences for each age group in 2020 assuming that those prevalences remained constant at the values that age group would have had in the past when it was aged 15-24. Comparing this with the actual prevalences for 2020 allows estimation of the proportion of the change in prevalence over time that is attributable to cohort effects.
For practicing religious, non-religious and atheists, the cohort projection explains around 25% of the overall change, the other 75% is attributable to period. For the non-practicing religious, these proportions are reversed with 25% explained by period and 75% by cohort.
Projecting religiosity prevalences to 2030
My previous projections of religiosity to year 2020 were carried out using trends in all-ages-both sexes prevalences. I thought it would be interesting to explore projections at age-sex level for selected countries, given the likely variations in trends across age groups. I experimented with several statistical models including a period-cohort projection model, and a model that projected all four prevalences simultaneously, using seemingly unrelated regression techniques to constrain the prevalences to add to 100%. It proved difficult to get sensible results from these models when not tailored to specific country data. The disaggregation of survey data to 7 age groups for each sex resulted in highly variable prevalences across cells. The years for which surveys were available varied across countries in ways that made it difficult to develop generalized projection methods that were not sensitive to small number issues and outlier trends.
I eventually decided to do some quite simplistic projections for each age-sex category as follows:
Project from last available wave to 2022 using short-term trends given by last two waves
Project from 2022 to 2030 using longer-term trend from wave closest to year 2000 to last wave
Adjust extreme trends to either the smaller of the short and long run trends, or to trends for neigbouring age-sex groups.
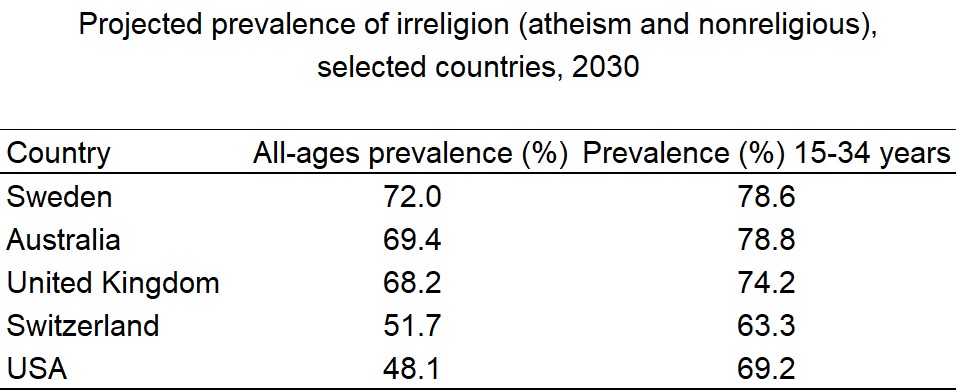
I carried out these projections for five high income countries with rising prevalence of atheism: USA, Australia, Switzerland, United Kingdom and Sweden. The following plots illustrate the observed and projected prevalences for the four religiosity categories. The dashed lines denotes the projected trend for irreligion (non-religious plus atheist).
The nonreligious category includes people who state that they believe in God, but that they are non-religious and rate the importance of God as 8-10 at the not important end of a 10-point scale. In the table below, I summarize the projected prevalence of irreligion (nonreligious or atheist) in 2030 for the five countries for all ages combined and for the young adult age group 15-34 years. The irreligion prevalence is generally higher in the younger age groups, and the 2030 value gives an indication of likely future trend for all ages.
Is irreligion likely to continue increase in the future? If the economies of high income countries continue to grow, with decreasing levels of poverty, and education levels continue to improve, it is likely that religiosity in these countries will decline in the longer term. The joint global crises of global warming and the pandemic, with rising populism and rejection of global institutions and actions, may on the other hand result in economic downturns that result in a stalling or reversal of the current religiosity trends. The situation in the USA where a religious minority is actively seeking to impose its values on the entire population, and undermining the democratic system to achieve that, may likely accelerate the turning away from religion of the young adult population. The USA already has one of the fastest rates of increase of irreligion in the last decade.
References
EVS (2021): EVS Trend File 1981-2017. GESIS Data Archive, Cologne. ZA7503 Data file Version 2.0.0, https://doi.org/10.4232/1.13736
EVS/WVS (2021). European Values Study and World Values Survey: Joint EVS/WVS 2017-2021 Dataset (Joint EVS/WVS). JD Systems Institute & WVSA. Dataset Version 1.1.0, doi:10.14281/18241.14.
Haerpfer, C., Inglehart, R., Moreno, A., Welzel, C., Kizilova, K., Diez-Medrano J., M. Lagos, P. Norris, E. Ponarin & B. Puranen et al. (eds.). 2021. World Values Survey Time-Series (1981-2020) Cross-National Data-Set. Madrid, Spain & Vienna, Austria: JD Systems Institute & WVSA Secretariat. Data File Version 2.0.0, doi:10.14281/18241.15.
In my previous post, I estimated that 47% of pregnancies are unintended, and of these, 43% occur in countries where abortion is illegal or severely restricted. In countries where abortion is widely available, 71% of unintended pregnancies are aborted compared to 46% in countries with severe restrictions.
The World Health Organization (WHO) estimates that around one-third of the 23 million induced abortions carried out each year in countries where abortion is severely restricted are performed under the least safe conditions, by untrained persons using dangerous and invasive methods. Safe abortion is an essential health care service. It is a simple intervention that can be effectively managed by a wide range of health workers using medication or a surgical procedure. In the first 12 weeks of pregnancy, a medical abortion can also be safely self-managed by the pregnant person at home.
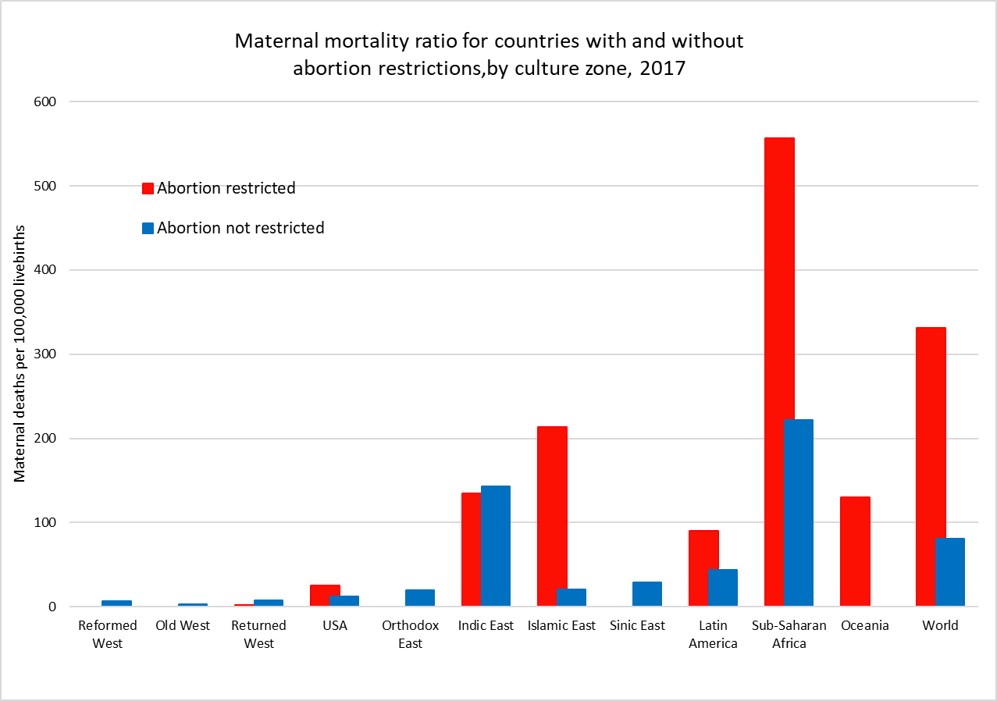
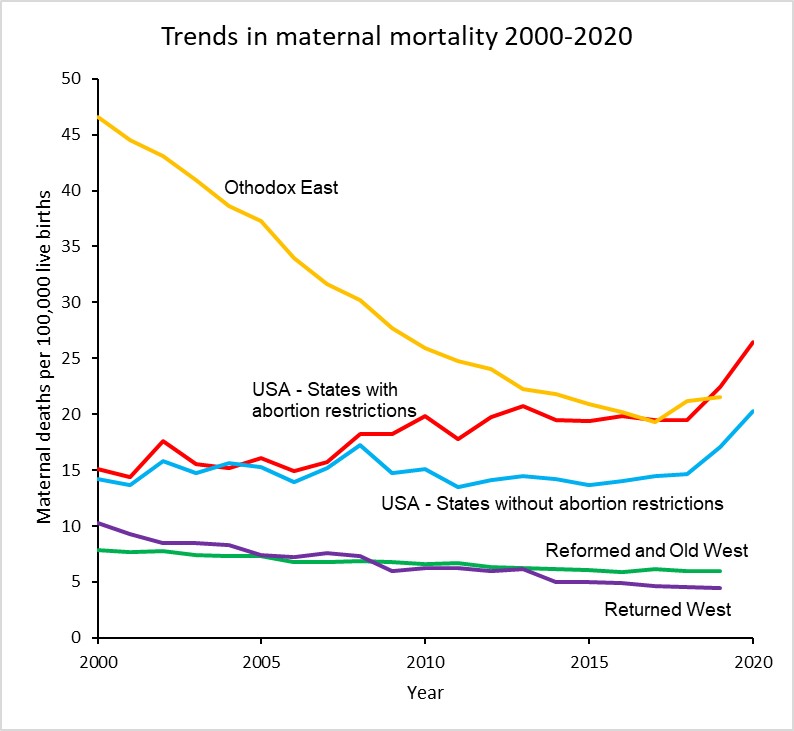
Maternal mortality is defined as death while pregnant or within 42 days of the end of pregnancy from any cause related to or aggravated by the pregnancy or its management. The plot above shows the average maternal mortality ratio (MMR) per 1,000 live births for countries (and US states) grouped by access to abortion and culture zone for the year 2017 (see here for more details).
While countries that restrict abortion have higher MMRs than those that don’t for most of the culture zones, we cannot conclude that abortion restriction per se is responsible for the difference. Abortion restriction is also correlated with other determinants of higher MMR such as lower average income per capita, less access to health care, and higher levels of discrimination against women.
The global MMR has declined from 345 per 100,000 livebirths in 2000 to 212 per 100,000 livebirths in 2017, a 40% decrease in 17 years. There have been substantial declines in MMR in every culture zone except for the Reformed West and Old West where MMR rates were already very low in 2000 and in the USA where rates have risen substantially during the 21st century.
The plot below takes a closer look at MMR trends in the USA, the Reformed and Old West, the Returned West and the Orthodox East. The latter two culture zones include the former Soviet bloc countries. With the exception of Poland in the Returned West, all these culture zones except the USA do not restrict access to abortion services and allow abortion on request or in some countries on “economic and social grounds”.
The maternal mortality ratio for the USA has increased from around 15 per 100,000 livebirths in 2000 to 23.8 in 2020, a 62% increase. Abortion rates in States which now restrict abortion were similar to those in states which don’t until 2008 and afterwards diverged substantially. The rate for states with restrictions was 26.4 in 2020, 30% higher than the MMR of 20.2 for states without restrictions.
There has been considerable controversy about the substantial increase in maternal mortality in the USA, particularly as to whether it is associated with improvements in the identification and reporting of maternal deaths. The addition of a pregnancy checkbox to death records from 2003 onwards is thought to have led to some increase in estimated MMRs in the early 2000s, but several studies have also identified that increasing restrictions on the general availability of reproductive health services have played a major role, particularly in states restricting access to abortion.
Hawkins et al (2019) found that a 20% reduction in the numbers of Planned Parenthood clinics resulted in an 8% increase in maternal mortality and states that enacted legislation to restrict abortions based on gestational age increased the maternal mortality rate by 38%.
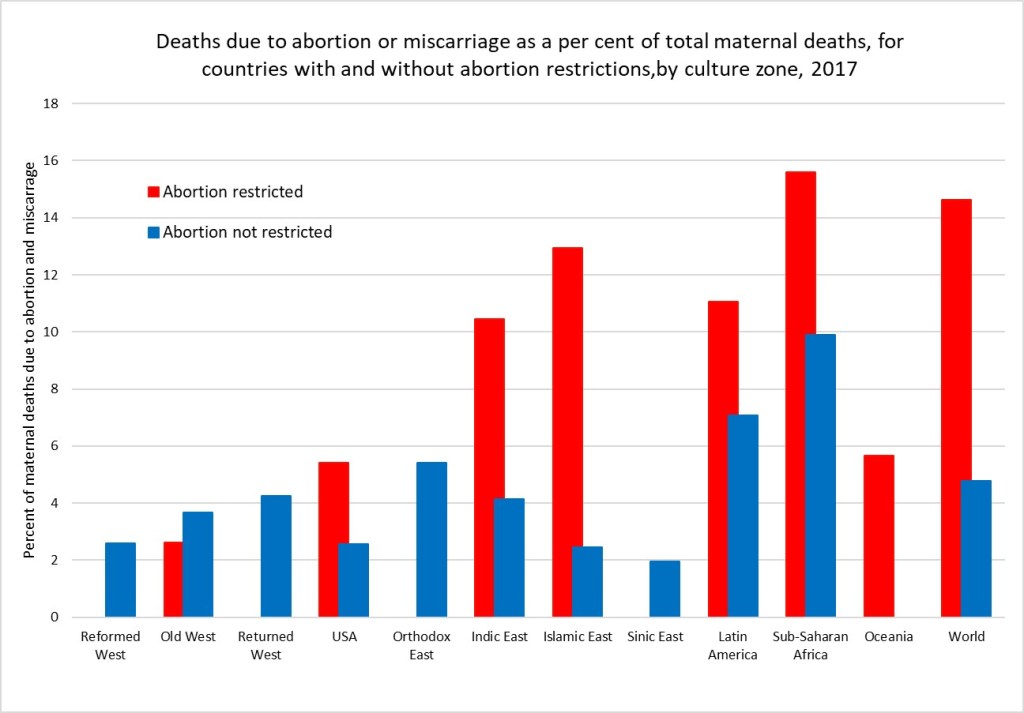
A 2020 study by the Commonwealth Fund compared maternity care in the USA with 10 other developed countries and found that the USA has the highest maternal mortality among developed countries and that there is an overall shortage of maternity care providers (obstetrician-gynecologists and midwives). The USA has 12 to 15 providers per 1,000 livebirths, and all the other developed countries have a supply that is between two and six times greater. Although a large share of its maternal deaths occur postbirth, the U.S. is the only country not to guarantee access to provider home visits or paid parental leave in the postpartum period. In the early 2000s, WHO estimated that unsafe abortion accounted for around 13% of total global maternal deaths, then estimated to be around half a million deaths per year. A more recent study by WHO staff and academic colleagues in 2014 estimated that abortion accounted for 7.9% of maternal deaths at global level between 2003 and 2009. Recent WHO estimates for global deaths by cause do not include deaths due to induced abortion. I have elsewhere used results from the Global Burden of Disease Study 2019 to estimate very approximately the proportion of maternal deaths due to abortion and miscarriage for the period 2015-2019. These would include induced abortion deaths as well as deaths due to spontaneous abortions and miscarriages. The following plot shows the estimated average percent of maternal deaths attributed to abortion and miscarriage for countries with and without abortion restrictions in each culture zone.
Overall, I estimate that there were 75,500 deaths globally due to abortion and miscarriage in 2017 (these include spontaneous events as well as induced abortions). Of these 70,300 were in countries with abortion restrictions. Assuming the rate in countries with unrestricted abortion relates to the spontaneous events, I have estimated that abortion restrictions resulting in unsafe abortions caused 54,350 deaths in 2017. If all abortions were safe, there would have been only 21,200 deaths globally due to spontaneous abortion and miscarriage in 2017.
Its quite possible these very back-of-the-envelope estimates are under-estimates. Classification of maternal deaths due to abortion, and more specifically unsafe abortion, is associated with a risk of misclassification. Even where induced abortion is legal, religious and cultural perceptions in many countries mean that women do not disclose abortion attempts and relatives or health-care professionals do not report deaths as such.
A medical abortion procedure uses the drugs mifepristone and misoprostol which can be taken in pill form up until the 12th week and are very safe.They require no surgery or anaesthesia. These drugs were developed in 1980 and first became available for induced abortions in France in 1987. It became available in the USA in 2000 and is on the WHO list of essential medicines. Cost and availability limits access in many parts of the developing world.
It is usually possible to carry out this procedure oneself at home. During the covid pandemic, a number of countries including the UK have made abortion accessible via an online consultation after which the pills are sent by post to the woman to take at home. The Netherlands-based charity Women on Web aims to prevent unsafe abortions by providing abortion pills to women in countries where safe abortion is available.
In December 2021, the FDA made permanent a covid-era policy allowing abortion pills to be prescribed via telehealth and distributed by mail in US states that permit it.Even before the FDA action,abortions induced by pills rose to more than 54 percent of all U.S. abortions in 2020, according to the Guttmacher Institute. Nineteen states have banned prescription of these pills via online consultation, requiring the woman visit a physician. And of course, in states which severely restrict abortion, this will require a completely unnecessary trip out of state.
Women on Web is making medical abortion available to women in the USA and elsewhere who are facing these restrictions. The cost for a woman to obtain the pills for a medical abortion is 90 Euros, or around 100 US dollars. You can donate to fund abortions for women unable to afford them here. Or to US based abortion funds here.
While legal abortions done under the guidance of a professional are the gold standard. Self-managed abortion can be safe, too, if you have the right information. But as I noted above, the banning of abortion typically goes hand-in-hand with restrictions on contraception and reproductive health services, as well as discrimination and other restrictions on women that result in higher maternal mortality rates, more femicide and abuse, less access to education and employment, and greater female poverty levels.
The removal of a basic reproductive rights for women in the USA is being driven by a minority, many of whom are fundamentalist Christians. According to a recent survey, white and Hispanic fundamentalists are the only religious group in the USA for which a majority oppose the legal availability of abortion (The Economist, May 7, 2022).
I discussed in a previous post how enforcement of social norms governing human fertility have been a major factor in pre-modern religions. For thousands of years, very high levels of child mortality and other survival pressures meant that most societies sought to ensure that women produced as many children as possible and discouraged divorce, abortion, homosexuality and contraception. Additionally sexual behaviour, particularly that of women and that not linked to reproduction, was strongly socially controlled to minimise uncertainty about paternity. Religion was the primary method of social control and pre-modern values regarding women’s rights, reproduction and sexuality are still dominant in most of the major religions, particularly fundamentalist forms. In a world facing overpopulation, global warming, habitat destruction and species extinction, it is crucial that outdated and cruel pre-modern values do not condemn women to reproductive slavery and an inability to control their own fertility, and reduce our ability to address these inter-related crises using all the tools and knowledge now available.
Many of us here in Europe and Australia are watching in horror as the US Supreme Court moves towards taking away the reproductive freedom of US women. And from the noises being made by Republican politicians, access to contraceptives, gay marriage and any other human rights not recognized in the 16th century are at risk also.
During my close to two decades responsible for WHO global health statistics, I worked closely with the maternal health department on regular assessments of maternal mortality, including deaths due to unsafe abortion. My team collaborated with the Guttmacher Institute on several occasions to produce global statistics on induced abortion. Given the current situation, I was interested to see that the Guttmacher Institute and WHO released first-ever country-level estimates of unintended pregnancy and abortion (see here) a little under two months ago.
The new study analysed data for 150 countries for the period 2015-2019, and found that:
Almost half of the 220 million pregnancies globally per year are unintended.
Six in 10 unintended pregnancies end in an induced abortion (63 million per year).
Overall, 29% of all pregnancies globally end in an induced abortion.
Regional averages mask large disparities within regions for unintended pregnancy and abortion rates.
The Guttmacher/WHO study covers 90% of the 1.9 billion women of reproductive age. Almost all the missing countries (because of lack of data) are in the Western Asia and Northern Africa region, most of them Islamic states or with a dominant Islamic culture. I describe elsewhere how I imputed data for most of the missing countries and added data on legal grounds and restrictions regarding abortion. Countries classified as having abortion restrictions are those which completely prohibit abortion or allow abortion only on one or more of the following grounds: risk to life, risk to health, rape or fetal impairment. Countries classified as without abortion restrictions also allowed abortion on social or economic grounds, or on request. Given the polarization of the US states in allowing or restricting abortion, I also used information from Planned Parenthood to classify US states into two groups with and without restrictions.
First, a brief overview at the global level of the differences between grouped countries with and without restrictions:
36% of women of reproductive age live in countries with restricted access to abortion. These countries account for 33% of global abortions, 50% of global live births and 81% of global maternal deaths.
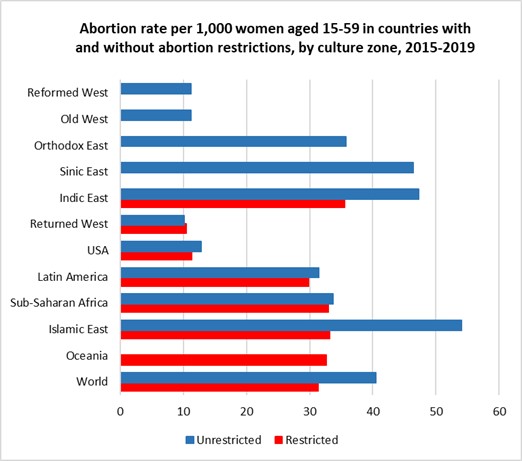
The global abortion rate per 1,000 women aged 15-49 years is 31 for countries with restrictions and 41 for countries without restrictions.
21% of pregnancies are terminated by abortion in countries with restrictions, 34% in countries without restrictions.
Average GDP per capita (purchasing power parity dollars) was $18,300 in countries without restrictions, and 71% of women aged 15-49 used modern forms of contraception. For countries with restrictions, the average GPD/capita was $8,500 and only 57% of women used modern forms of contraception.
Countries restricting abortion were much more religious with 66% of adults attending religious services at least once a month, compared to 27% in countries not restricting abortion (data on religious practice from the World Values Survey and European Values Study, see earlier post here).
These global averages conceal very large differences across regions, and between countries in some regions. I have examined these patterns by grouping countries into 11 culture zones, based on those developed by Welzel (2013) for the World Values Survey.
I modified the culture zones slightly, to include Canada in the Reformed West and keep the USA in its own separate category. I also moved predominantly Muslim countries from “Indic East” and “Sinic East to group together all countries with a predominantly Islamic culture and values. See here for full definitions of the culture zones.
Figure 1
Figure 2.
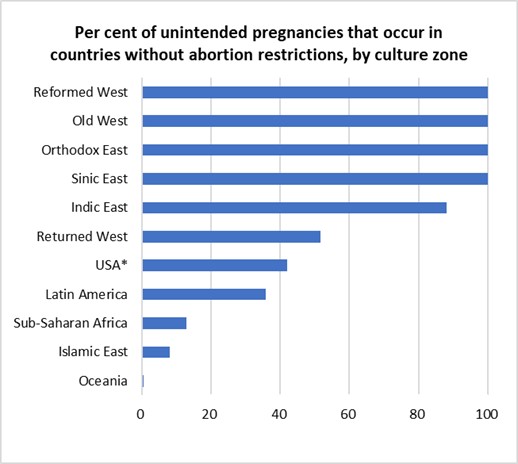
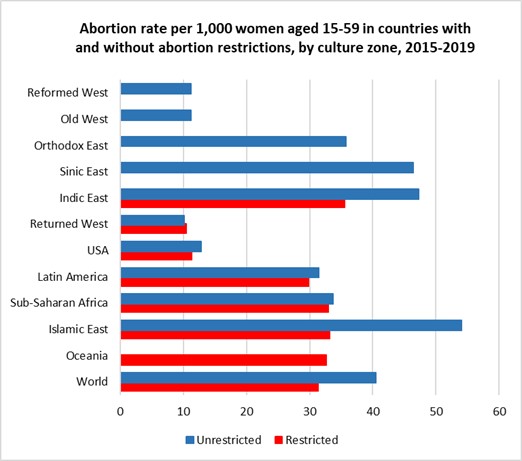
The left-hand figure 1 shows that abortion is universally legally available in most of Europe, Canada, Australia and New Zealand, in the Orthodox and Islamic countries of the former Soviet-bloc and in the non-Islamic countries of Asia. It is legally severely restricted in most Islamic countries and sub-Saharan Africa. Abortion rates are substantially lower in the high-income countries of Europe, North America and Australia and New Zealand than in the Asian regions where abortion is unrestricted AND in the countries in all developing regions irrespective of whether abortion is legally restricted or available. Note that USA results have been calculated by grouping States into those with and without significant abortion restrictions.
For 2015-2019, almost half of unintended pregnancies (46%) were aborted in countries where abortion was restricted (often severely) and a little over two-thirds (70%) in countries where abortion is accessible. In the three regions where around 40-50% of women with unintended pregnancies have restricted access to abortions, overall abortion rates per 1,000 women of reproductive age differ by less than 2 abortions per 1,000 from those in countries (or US states) without restrictions. These are the USA (11 versus 13 per 1,000), the Returned West (11 versus 10 per 1,000) and Latin America (30 versus 31 per 1,000). The Returned West consists of former Soviet-bloc countries that have joined the EU, and the largest of these, Poland, is the only one to have restricted abortion, prohibiting it for fetal impairment, economic or social reasons, or on request.
People seek and obtain abortions in all countries, even in those with restrictive abortion laws, where barriers to safe abortion care are high. In fact, over the past three decades, the proportion of unintended pregnancies that end in abortion has increased in countries that have many legal restrictions in place. The figures presented above suggest that the illegalization of abortion will not substantially reduce its incidence. Over recent decades, most of the changes to the legal grounds for abortion have been in the direction of recognizing women’s rights to reproductive autonomy (recent examples include Ireland, Argentina, Mexico and Columbia).
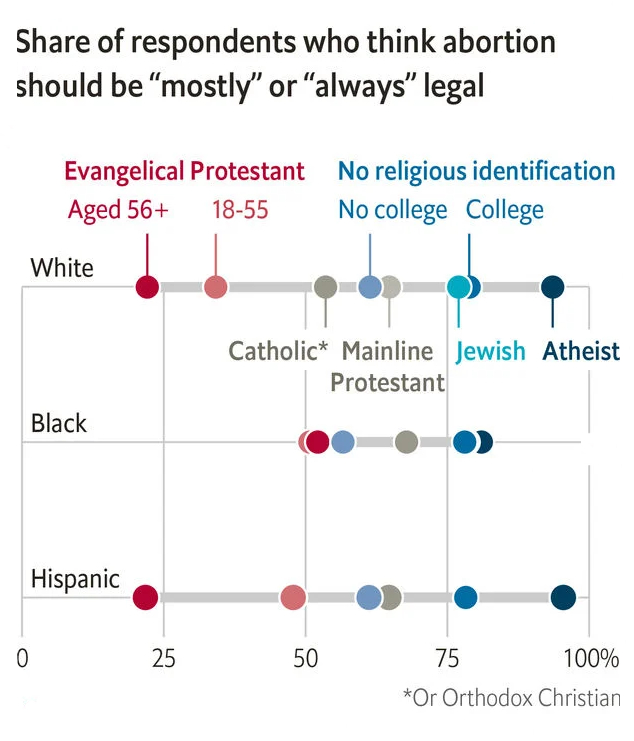
The increasing restrictions in the USA are one of the few examples of major reductions in women’s rights occurring outside the Islamic countries. In the case of the USA, these changes are to rights that women have had for half a century and are being driven by an anti-democratic coalition of white nationalists and religious extremists who do not represent the majority views of the population. A recent issue of the Economist identified white evangelicals as the one major religious group with majority opposition to the legal availability of abortion (The Economist, May 7, 2022). A majority of Catholics, mainline Protestants and those with no religious identification think that abortion should be mostly or always legal in the USA, and support is over 75% for Jewish, atheists and non-religious with college education.
The rhetoric of some US extremists, and actions already taken to restrict health insurance coverage for contraceptive use, suggests that further restriction on abortion access may well also be accompanied by further reductions in contraceptive availability. The unintended pregnancy rate may well increase, resulting in an overall increase in numbers of abortions occurring, even if the restrictions reduce the percentage of unintended pregnancies that end in abortion. In my next post, I will examine differences in maternal mortality across countries and the extent to which they are associated with legal restrictions on abortion.
A little under two months ago, the Guttmacher Institute and WHO released first-ever country-level estimates of unintended pregnancy and abortion (see here). The new study analyzed data for 150 countries for the period 2015-2019 and found that:
Almost half of the 220 million pregnancies globally per year are unintended.
Six in 10 unintended pregnancies end in an induced abortion (63 million per year).
Overall, 29% of all pregnancies globally end in an induced abortion.
Almost 30% of induced abortions occur in countries where abortion is either illegal or heavily restricted. Earlier estimates for 2010-2014 found that 45% of all abortions are unsafe, and around 15% were performed in the least safe conditions, by untrained persons using dangerous and invasive techniques.
Regional averages mask large disparities within regions for unintended pregnancy and abortion rates.
The Guttmacher/WHO study covers 90% of the 1.9 billion women of reproductive age. Almost all the missing countries (because of lack of data) are from the Western Asia and Northern Africa region, most of them Islamic states or with a dominant Islamic culture. I describe below how I imputed data for most of the missing countries, added data on legal grounds and restrictions regarding abortion and examine global patterns using 12 culture zones which group countries based on history, values and religion.
The following plots give a taste of the global patterns I found. Culture zone and other definitions, data and methods are given in more detail in the rest of this post.
Figure 1.
Figure 2.
*Note that USA results have been calculated by grouping States into those with and without significant abortion restrictions
The left-hand figure shows that abortion is universally legally available in most of Europe, Canada, Australia and New Zealand, in the Orthodox and Islamic countries of the former Soviet-bloc and in the non-Islamic countries of Asia. It is legally severely restricted in most Islamic countries and sub-Saharan Africa. Abortion rates are substantially lower in the high-income countries of Europe, North America and Australia and New Zealand than in the Asian regions where abortion is unrestricted AND in the countries in all developing regions irrespective of whether abortion is legally restricted or available. Note that USA results have been calculated by grouping States into those with and without significant abortion restrictions.
For 2015-2019, almost half of unintended pregnancies (46%) were aborted in countries where abortion was restricted (often severely) and a little over two-thirds (70%) in countries where abortion is accessible. In the three regions where around 40-50% of women with unintended pregnancies have restricted access to abortions, overall abortion rates per 1,000 women of reproductive age differ by less than 2 abortions per 1,000 from those in countries (or US states) without restrictions.
Imputation of data for countries in Western Asia and Northern Africa
The 150 countries with abortion-related data represent 90% of the 1.9 billion women of reproductive age 15-49 years in the period 2015-2019. Of the eight Sustainable Development Goals (SDG) regions used in the study, the coverage of reproductive-age women by countries with data fell below 95% only for Western Asia and Northern Africa, where data coverage was only 3.4%. However, the missing women are almost entirely in one SDG region, Western Asia and Northern Africa
The region includes 24 countries, mostly in North Africa and the Middle East. Data is available only for Azerbaijan, Armenia and Georgia. These are all former Soviet-bloc countries with legal abortion and high rates of termination of unintended pregnancies. In contrast, apart from Israel and Cyprus, the other 19 countries are all either explicitly Islamic states or with a predominant Islamic culture. Seventeen of the 19 either prohibit or severely restrict abortion.
To address the bias inherent in excluding these countries from global statistics, I decided to impute the unintentional pregnancy rates and abortion rates for the Islamic countries in North Africa and the Middle East and also for Afghanistan, Iran and Malaysia, using information on live birth rates for these countries along with the abortion data for 22 Islamic countries in the neighbouring regions Sub-Saharan Africa, South-central Africa and South-eastern Asia. Former Soviet-bloc Islamic countries were not included in this dataset.
Pregnancy rates were regressed against live birth rates for this dataset and the regression model (R-squared 0.91) used to predict pregnancy rates for the missing data. Unintended pregnancies are defined as pregnancies which were unwanted at the time they were conceived or occurred earlier than desired. Explorations of various covariates for predicting the proportion of pregnancies that are unintentional resulted in predicting of missing data using a regression on the log of GDP per capita measured in international (purchasing-power-parity adjusted) dollars and a continuous variable measuring average-religiosity for countries in 2017. Both these variables are significant predictors of the proportion of pregnancies that are unintentional and the regression on the prediction dataset has an R-squared of 0.52. I used previously estimated levels and trends in average religiosity (practicing, non-practicing, non-religious and atheist) for countries using data from the World Values Survey (WVS) and European Values Study (EVS) covering the period 1980 to 2020 (see previous post here).
The only predictive variable found for the proportion of unintentional pregnancies resulting in induced abortion was the gender inequality index produced by United Nations Development Program. Regression of logit(abortion fraction of unintended pregnancies) against the logit of the 2017 value of the gender inequality index was used to predict missing abortion fractions of unintended pregnancies (R-squared 0.7).
Global and regional abortion rates for 2015-2019
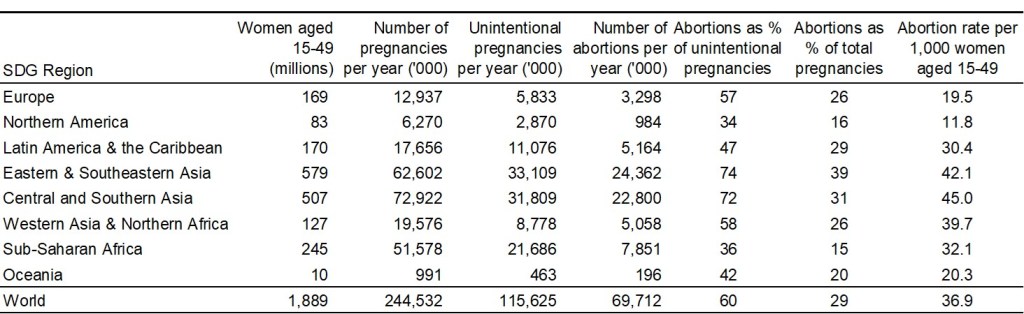
With these missing values imputed for 23 countries, the abortion estimates now cover most countries in most regions, and 98.6% of women of reproductive age globally. Based on this extended dataset, the following table summarizes regional and global patterns of pregnancy and abortion for the period 2015-2019.
The Guttmacher/WHO paper in the British Medical Journal displays unintended pregnancy and abortion rates by country for the 150 countries included in their study. The estimates dataset is available here. It includes 80% and 95% uncertainty intervals. In this post, I’m interested to see the big picture at regional and global level, and I’ve not done the additional work to estimate uncertainty intervals. But it is important to keep in mind that there are many problems with data availability, reliability and completeness of reporting, particularly for an often stigmatized and contentious issue such as abortion. So the broad patterns shown below likely convey a reasonable and evidence-based assessment, but small differences between countries or regions should not be over-interpreted.
Legal restrictions in countries and US States
The legality and acceptability of abortion varies widely across the world, from Europe where it is available without restriction in most countries, to the Middle East and Africa where it is largely illegal.
I’ve taken country-level information on abortion availability and restrictions from Wikipedia, which documents legal grounds on which abortion is permitted, and gestational age limits where relevant, using the following six categories: risk to life, risk to health, rape, fetal impairment, economic or social reasons, on request. The first four of these grounds cover a fairly small percentage of unintended pregnancies and I have grouped in a single category “restricted or prohibited” countries which allow abortion only on these grounds. Countries which allow abortions on economic or social grounds or on request (with any gestational age limit set at least 10 weeks or longer) are classified as “unrestricted”. The USA has widely varying legal restrictions on abortions across the 50 states and Washington DC. I have used information on abortion access from Planned Parenthood to classify abortion access as restricted (28 states) and unrestricted (22 states and Washington DC).
Revised culture groups for countries
In earlier posts, I analyzed religious and other values by culture groups for 110 countries using data from the World Values Surveys and the European Values Study. These culture zones were based on the 11 culture zones developed by Welzel (2013).
For this post, I’ve slightly revised the culture zones to group Canada with Australia and New Zealand in the “Reformed West” zone, and kept the USA as a single separate culture zone. I’ve also revised the categories “Indic East”, “Sinic East”, and Islamic East to group together all countries with a predominantly Islamic culture and values. The revised culture zones are as follows:
Reformed West — Western European societies strongly affected by the Reformation: Denmark, Finland, France, Germany, Iceland, Netherlands, Norway, Sweden, Switzerland, United Kingdom, plus Canada, Australia and New Zealand;
USA — The North American culture zone included only two countries, USA and Canada. Canada’s culture is very similar to the Reformed West, and it is moved there.
Old West — Mostly Catholic parts of Western Europe being core parts of the Roman Empire: Austria, Belgium, Cyprus, Greece, Ireland, Israel, Italy, Luxembourg, Malta, Portugal, Spain;
Returned West — Catholic and Protestant parts of post-communist Europe returning to the EU: Croatia, Czechia, Estonia, Hungary, Latvia, Lithuania, Poland, Slovakia, Slovenia;
Orthodox East — Christian Orthodox or Islamic parts of the post-communist world, mostly parts of former USSR;
Indic East — Parts of South and South East Asia under the historic influence of Indian or Buddhist culture: Bhutan, Cambodia, India, Laos, Malaysia, Myanmar, Nepal, Philippines, Singapore, Sri Lanka, Thailand, Timor-Leste;
Islamic East — Countries with predominantly Islamic religion and culture;
Sinic East — Parts of East Asia under the historic influence of Chinese culture and/or Buddhism: China, Japan, Mongolia, North Korea, South Korea, Taiwan, Vietnam;
Latin America — Central and South America and the Caribbean;
Sub-Saharan Africa — African countries south of the Sahara.
Oceania — Papua New Guinea and other Pacific Island countries.
Patterns of abortion by culture group
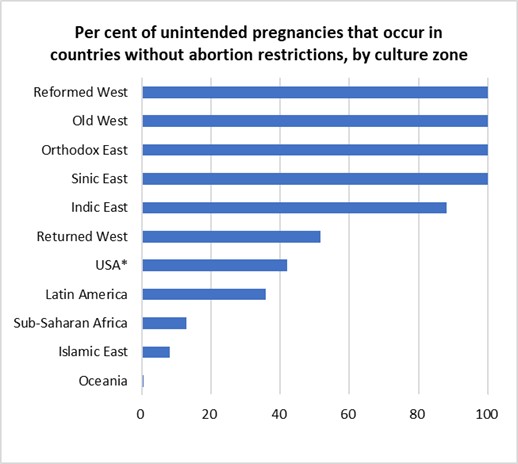
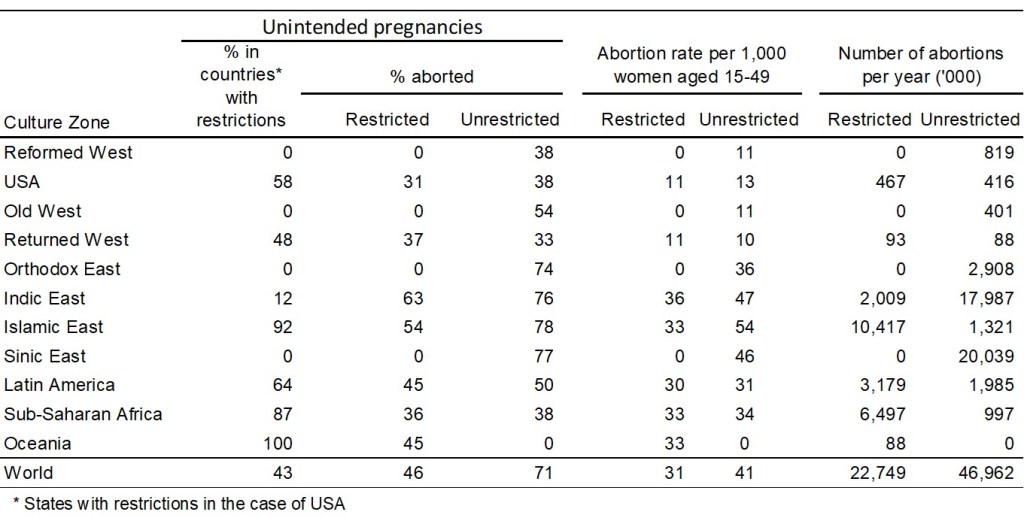
The table below summarizes the abortion situation for countries without legal restrictions and countries with legal restriction in each culture zone. Country-level legal status is used except for the USA where the statistics relate to two groups of states: those with and without legal restrictions on abortion (as defined above). State level estimates are not available for the per cent of unintended pregnancies, or the per cent that are aborted. I have assumed that the national percent of all pregnancies that are unintended (34%) is the same in the two groups of states, and that the % aborted in states without restrictions is the same (38%) as that in the Reformed West where abortion is 100% unrestricted. Since the national level of unintended pregnancies that are aborted is 34%, this implies that the proportion of unintended pregnancies aborted in states with restrictions is 31%.
To graphically illustrate these variations across culture zones, I repeat the two figures included near the beginning of this post:
Figure 1.
Figure 2.
Globally, 60% of unintended pregnancies ended in abortion in the period 2015-2019. People seek and obtain abortions in all countries, even in those with restrictive abortion laws, where barriers to safe abortion care are high. In fact, over the past three decades, the proportion of unintended pregnancies that end in abortion has increased in countries that have many legal restrictions in place. For 2015-2019, almost half of unintended pregnancies (46%) were aborted in countries where abortion was restricted (often severely) and a little over two-thirds (70%) in countries where abortion is accessible.
In the three regions where around 40-50% of with unintended pregnancies have restricted access to abortions, overall abortion rates per 1,000 women of reproductive age differ by less than 2 abortions per 1,000 from those in countries (or US states) without restrictions. These are the USA (11 versus 13 per 1,000), the Returned West (11 versus 10 per 1,000) and Latin America (30 versus 31 per 1,000). The Returned West consists of former Soviet-bloc countries that have joined the EU, and the largest of these, Poland, is the only one to have restricted abortion, prohibiting it for fetal impairment, economic or social reasons, or on request.
The figures presented above suggest that the illegalization of abortion will not substantially reduce its incidence. Over recent decades, most of the changes to the legal grounds for abortion have been in the direction of recognizing women’s rights to reproductive autonomy (recent examples include Ireland, Argentina, Mexico and Columbia). Removal of a right that women have had for 50 years in the USA is an entirely different situation.
The increasing restrictions in the USA are one of the few examples of major reductions in women’s rights occurring outside the Islamic countries where religious extremists have taken control of government. In the case of the USA, these changes are to rights that women have had for half a century and are being driven by an anti-democratic coalition of white nationalists and religious extremists who do not represent the majority views of the population. A recent issue of the Economist identified white evangelicals as the one major group with majority opposition to the legal availability of abortion. A majority of Catholics, mainline Protestants and those with no religious identification think that abortion should be mostly or always legal in the USA, and support is over 75% for Jewish, atheists and non-religious with college education.
Reproduced from: Religion, not gender, is the best predictor of views on abortion.The Economist, May 7th 2022.
The rhetoric of some US extremists, and actions already taken to restrict health insurance coverage for contraceptive use, suggests that further restriction on abortion access may well also be accompanied by further reductions in contraceptive availability. The unintended pregnancy rate may well increase, resulting in an overall increase in numbers of abortions occurring, even if the restrictions reduce the percentage of unintended pregnancies that end in abortion.
In my next post, I will examine differences in maternal mortality across countries and the extent to which they are associated with legal restrictions on abortion.
Mary Beard covers what she calls the first thousand years of Roman history from around 753 BCE, the traditional date of the founding of Rome by the mythical Romulus and Remus, through to 232 CE when the Emperor Caracalla made every single free inhabitant of the Roman Empire a full Roman citizen. Unlike many histories which focus on the so-called decline and fall of the Roman Empire during the following period through to around 476 CE, when the Gothic Odoacer deposed the last Emperor and declared himself King of Italy, Beard attempts to examine the question of how one tiny and unremarkable Italian village became so dominant a power over so much territory in three continents.
In recent weeks, I’ve been reading SPQR: a history of Rome by Mary Beard (2015) and simultaneously dipping into the classic The Origins of Totalitarianism by Hannah Arendt (1951). Hannah Arendt in much slower going and about halfway into SPQR I became so engrossed I just binge read to the end.
Mary Beard covers what she calls the first thousand years of Roman history from around 753 BCE, the traditional date of the founding of Rome by the mythical Romulus and Remus, through to 232 CE when the Emperor Caracalla made every single free inhabitant of the Roman Empire a full Roman citizen. Unlike many histories which focus on the so-called decline and fall of the Roman Empire during the following period through to around 476 CE, when the Gothic Odoacer deposed the last Emperor and declared himself King of Italy, Beard attempts to examine the question of how one tiny and unremarkable Italian village became so dominant a power over so much territory in three continents.
I was in high school during the 1960s and psychedelics were illegal by the time I started university in 1971. Although I was fascinated by writings on psychedelics by Aldous Huxley, Alan Watts and others, and the experiences recounted by various friends, my fear of adverse outcomes led me to avoid trying LSD when the opportunity presented.
In 2019, I read several accounts of people who had attended legal psychedelic retreats in the Netherlands and elsewhere seeking to facilitate personal development. I also read Michael Pollan’s best-selling book on the current psychedelic renaissance, Changing Your Mind. I was searching for new priorities and purposes in life after divorce and retirement. Maybe a psychedelic retreat could provide some clarity?
So I decided to attend a psychedelic retreat and this is an account of my experiences. They led in an altogether unexpected direction and led to the resolution of repressed trauma that I had been unaware of.
Legal retreats in the Netherlands
The Netherlands fully legalized the psilocybin-containing truffle form of magic mushrooms in 2019 and a number of organizations started to provide psychedelic retreats designed to facilitate personal growth, emotional breakthroughs and spiritual development. There is growing evidence for the transformative potential of a well-prepared psychedelic experience in a safe and supportive environment (see for example Madsen et al 2020, Aday et al. 2020, Kettner et al. 2021). . A new wave of research is also finding that psychedelics can offer significant therapeutic benefits for people suffering with depression, trauma or addiction (see here and here).
The Synthesis retreat centre in Amsterdam has been running 3 day retreats since April 2018. After speaking to several retreat facilitators at Synthesis, I decided to enrol for their first five-day retreat in October 2019. This would include two psilocybin ceremonies on the second and fourth day. Before enrolment, I undertook an interview and a health screening process, similar to that being used in clinical studies of psilocybin.
I also accepted an invitation to participate in a research study being carried out by the Centre for Psychedelic Research at Imperial College London to investigate changes in wellbeing associated with the retreat process. This involved answering questionnaires at six different points in time; before, during and after attending the retreat, as well as wearing a bracelet during the retreat days to monitor various physiological variables.
Synthesis puts a strong emphasis on preparation before the retreat, support from facilitators during the retreat, and integration of the experience and its lessons into daily life after the retreat. The three-week preparation phase included weekly group Zoom calls and preparatory activities including journaling, meditation and the development of three intentions for the retreat. These intentions play a crucial role as the expectations of the psychedelic voyager usually have a strong influence on what is experienced. My two main intentions were: to reach closure on the end of my marriage, and to clarity on my goals and priorities in retirement. My third intention was more of a wishful hope that I would experience the ego-dissolution that psilocybin can cause, and that I had previously experienced several times when practicing Zen meditation.
The first day at the retreat – flight instructions
The retreat was held in a converted church in near Amsterdam, now decorated in a mix of Buddhist and shamanic symbolism. There were around ten of us, together with five guides. We came from Europe, UK and North America and ranged in age from around twenty up to me in my sixties. Most of us had not had any previous experience with psilocybin.
Each of us was paired with an individual guide who would help us prepare for and integrate our psychedelic experience. My guide emphasised the importance of being open to the experience and not resisting it. He recommended that I work on this in the breathwork sessions later that day and the next morning.
The guides also gave us “flight instructions”: advice on the process, what to expect, and what to do if the experience became uncomfortable. They emphasised the importance of our three intentions in creating expectations that would influence psychedelic experience and maximize its potential benefits. We were given a mantra “Trust, let go and be open” to use when we recognized that we were resisting. The first ceremony would be a medium dose of psilocybin followed during the second ceremony by a deeper dive if requested.
First ceremony
The second day started with silent meditation and then a guided breathwork session to further prepare us for the afternoon ahead. The breathwork surprised me by releasing some quite strong emotions, resulting in tears and bodily shaking, and I used the mantra to stay open to the experience.
After a light lunch, we prepared the truffle tea. We ground up truffles and ginger, then added boiling water to make a ginger tea. Mattresses were arranged in a large circle in the ceremony room, each with pillows and a gravity blanket. When everyone was settled on their mattresses, we were served our truffle tea. I drank it all and then ate all the ground truffles left in the cup. I put on my blindfold mask, lay down on my back and covered myself with the gravity blanket as music from a curated playlist started to play. I was to lie there for the next five hours, apart from one trip to the toilet.
After maybe 15 or 20 minutes, I started to notice light and patterns. As I looked more closely these would break up and extend into intricate moving geometrical patterns or distinctive rainbow bands of colours shimmering and rippling. Every time I looked at something it would expand into fractals, or geometric patterns of immense detail and dynamics. I could drill down into these dynamic patterns and every level would expand.
And then my mind was totally caught up in the music. The music was much more than sound, it was colour, emotions, patterns, and very real and very solid. I experienced tones or chords as solid objects, that changed and grew with the music, building dynamic structures.
As the afternoon went on, the music and the visual patterns became less distracting. I started to get visions and to experience changes in my sense of self. I saw my parents and I was a child. I experienced myself as other people and even as four separate people.
I rummaged through the traumas of my life, revisiting periods when I was with my first wife and now-estranged daughters. I also revisited periods in my second long-term relationship. I re-experienced the love that I felt at those times, as well as the grief and sadness at the failures of those relationships. Curiously, the end of my most recent marriage did not come up.
When eventually I surfaced from my inner voyage and took the mask off, I looked at my hand. It looked gaunt and wrinkled and was going black and blue as I looked at it. When I went to the toilet and looked in the mirror, I saw an old man, a stranger, looking back at me.
I went back to the mat and kept drifting in and out of a meditative state, seeing difficult times in my life as if watching a movie, and still avoiding feelings. Towards evening, I went outside in the wind and watched the leaves and trees against the sky. I was cold but invigorated and feeling somewhat more open and connected.
Uncovering repressed feelings about my estranged daughters
On the third day of the retreat, I had a one-on-one session with my guide to understand and integrate the previous day’s experience, and to discuss strategies and intentions for the next day’s ceremony.
I was surprised that my trip had not focused on recent issues, but on the trauma and grief dating from the estrangement of my two daughters twenty years previously. I separated from my first wife in 1992 when my daughters were five and nearly eight. We divorced the following year and reached an agreement under which I had the girls about one-third of the time over the next seven years.
When I told my ex-wife in 1999 that I was going to work for a UN organization in Geneva for a year, she and my daughters refused any further contact. I have not seen them again since late 1999. Despite my close relationship with the girls, she convinced them that I was seeking to avoid my child support obligations. My efforts to show that I was not avoiding child support or seeking to avoid it were fruitless.
I was close to my daughters until they cut off contact, and the estrangement was hard for me to accept. I found a psychologist in Geneva and saw him for two or three years, reaching a point where I felt I had come to an acceptance of the situation and dealt with the grief and loss.
More recently I started counselling with another therapist about current issues and some of the emotions around the estrangement of the girls came up again. She spent time helping me to address that, and I thought I had reached acceptance of the situation and was no longer troubled by it.
Lying in bed falling asleep after the first ceremony, I became aware of the presence of buried feelings about my daughters’ estrangement. It felt as though they were encased in thick armour, like a spherical steel container. During the next day and night, I was always aware these encased feelings. It seemed like they were partly buried and partly protruding into my consciousness.
I very much wanted to get rid of this armour, to release whatever was inside. If I was ever going to explore what was buried deep inside my mind, this might just be the best place to do it. I determined to take advantage of the higher dose of truffles planned for the second ceremony to do this.
Second ceremony
We prepared the tea starting at 12 noon, this time with a higher dose of truffles. Almost immediately I was engrossed by extraordinarily intricate dynamic mandalas of bright lights, crystals, diamonds, endlessly unfolding, filling all space. I went deep into this space and was floating in front of an enormous spaceship. I felt I had a huge crushing weight on my chest and found that I stopped breathing unless I consciously took breaths. For a while I was worried that I would die if I forgot to breathe. Then I realized that I had guides sitting beside me and a medic nearby. They would notice if I wasn’t breathing, so I relaxed and stopped worrying.
The deep black space then transformed into an extraordinarily beautiful kaleidoscopic space filled with endlessly changing crystalline lights and colours. This went on so long that I started to worry. I wanted to go deeper and get past the light show to “important” stuff. I became very restless and repeatedly pulled off my blindfold.
My guide asked if I wanted more truffles and I said yes. After taking a second dose, about half the amount of the first, I put my mask and headphones back on. Now the music dominated and took me with it, and I started resenting it. I realized I was resisting, and said to myself several times “It’s me, don’t blame the music”. I then had a series of quite intense visionary experiences which became increasingly emotional. Some of these involved dramatic changes in the sense of self. I did not resist but leaned into the uncomfortable emotions that arose.
I saw my girls as they were when they were last with me. I experienced an intense feeling of loss and grief. Over and over, I said to myself “I miss you” as the feeling intensified. And at some point, I let go of the young girls and experienced the presence of my daughters as adults now. The grief transformed into love and I started crying and shaking.
One of the guides had noticed how overwhelmed with emotion I was, and sat next to me and held my hand, and his simple presence reassured me and encouraged me to open to my feelings.
After some time, I had an extended vision of the evolution of the universe, the earth, life, my ancestors and my place in the chain of life with my children following. And I saw myself getting very old and dying. I did not experience the dying itself but did experience that I was gone and that life goes on. And how crucial love is to that journey.
I was the last one left in the room by the time evening came. And still in an altered state. People came back into the room for a final closing and sharing circle. I was still there. Hadn’t left the room for close to 8 hours, apart from 2 trips to the toilet. On my second trip to the toilet, I looked in the mirror. Unlike in the first ceremony this time I saw a strong and healthy man looking back at me.
Integration
On the last day of the retreat I had another one-on-one session with my guide. I realized I had suppressed the feelings of loss, probably a decade ago, because they were too painful and had genuinely thought that I had accepted the situation. But in reality I was still caught up in the need to get the girls to realize they have been misled about me. Letting go of that need freed me from the anger and resentment I had been stuck in. My guide advised me to practice connecting with the deepest parts of myself and experience and express my love for all my children. That love is unconditional and does not depend on what the girls might believe. I don’t need to demand a response and the armour is gone.
We had weekly group video sessions over the next three weeks with the Synthesis guides to support and guide the integration process.
Two years later
After the retreat, I wrote letters to my daughters. I enclosed documentation of the child support payments made over the years. They can examine the facts if they want to. I no longer worry about what they might believe about me. I continue to write to them from time to time, so they know about my life and that I think about them and am open to communication.
I was somewhat disappointed that I did not have a profound no-self experience at the retreat or come home with clarity on what I wanted to do in retirement. It was not until around ten months later, when I volunteered to participate in a research study on the association of positive outcomes with psilocybin-induced experiences, that I realized that I had indeed had an extraordinary outcome, though not one I had anticipated. The pain and trauma that I had repressed, and did not know was still there, has now been replaced by openly experienced love accompanied by some sadness. Two psilocybin journeys in a supportive environment with appropriate integration has made a profound and long-lasting change, a change that I was not able to achieve through several years of psychological counselling. I feel like I’ve taken a very heavy weight off my mind and that has been incredibly liberating.
Research has shown that psychedelics have the capacity not only to retrieve past traumas, but to simultaneously dampen an overactive emotional response when it is relived. Even so, I doubt I would have had the courage to press through the resistance and repression if I had taken psilocybin on my own. My confidence that I was in safe surroundings with expert guides to assist if I got into difficulties allowed me to drop my resistance and surrender to the experience.
I have spent some time thinking about whether to share this deeply personal experience but decided it might be helpful to others to document my experience of the potential of psychedelics to resolve past traumas and issues.
I’ve had a number of near-death experiences over the years. Almost all of these were the result of sheer stupidity doing risky things. I recently read an account by someone who survived having seen certain death approaching. That and other recent circumstances have got me thinking about my own experiences and meditating on death and dying more generally.
In this post I remember two incidents in which I was knocked unconscious and would never have known about it if I had died. These experiences had a far greater impact on me and my feelings about death and dying than any of the incidents where I realized that death was a probable outcome.
The water slide in question
In the early 2000s, I was in South Africa for three weeks as one of the staff for a WHO global training course. The course was being held in a small game park and resort, which was closed to general visitors. There was a water slide which was also closed, but several of us persuaded the staff to open it one lunch time for us. The water slide was a fully enclosed tube with water running through it which ended over a small swimming pool about 2 metres deep. My friend J and I were the first two there and each did a slide down the tube. I sat up in the tube and found there was too much friction so that I went down quite slowly.
For my second slide, I lay down completely flat in the tube. I do now remember the initial moments, going quite fast and bouncing around in the tube. I must have hit my head on the side of the tube on the way down because I was unconscious when I entered the water and went to the bottom of the pool.
J had gone down before me and was already walking back up the path to the top of the slide. Halfway up he looked back and saw me lying on the bottom of the pool. He initially thought I was clowning around and kept walking. But when he looked back again, I was still in the bottom of the pool. He ran back down to pull me out of the water. I was bleeding heavily from a cut over one eye, and he told me later he thought my skull was broken and my brains were coming out. I regained consciousness a few minutes later, I don’t know whether he did resuscitation or I started breathing on my own. I asked him what happened and where was I. When he told me we were in South Africa, I was astonished. I had no memory of going to South Africa or any idea why I would be there. I was as astonished as if someone had just told me I was in Siberia. I knew who I was and who J was, but I had no memory of anything that had happened in the last few weeks.
An ambulance came, and I was taken to the nearest town with a hospital, where they took X-rays of my head and neck. And debated for some time whether the signs of fractures in my neck vertebrae were new or old (they were old). I was fitted with a neck brace and they stitched up the split skin over one eye. My amnesia gradually disappeared over a period of a day or so, until eventually I could remember the initial part of going down the slide and starting to oscillate. But the actual blow to the head and the aftermath before I came to has remained a blank.
After the accident
It was an existential shock to realize that if I had not been pulled out, but drowned, I would never have known. I would not have known I was about to die. Amnesia meant my mind was a blank in the minutes leading up to possible death. It was profoundly disturbing to realize it was entirely possible I would die without ever knowing about it. And it continues to be a realization that I keep revisiting.
I also realized that the state of being dead is nothing to fear. I experienced “not being there” in any form and its nothing at all to be afraid off. You don’t exist, and there is nothing to experience the not existing.
The second experience occurred a couple of years later in Geneva. I had left work to ride to the gym on my bicycle. I was riding in the bus lane on a road which went down a long slope from the World Health Organization. I was riding quite fast and became worried that a bus might be coming up behind me. I looked back and in doing so steered the bike into the gutter. I hit the gutter at speed and went over the front handlebars.
That is the last memory I have until I suddenly became aware that I was on my bicycle and covered in blood. I was bleeding quite profusely from skin loss on legs and arms and riding in heavy traffic. I had no idea where I was at all but knew from my injuries that I must have been in some sort of accident. I got off the bike and rang my wife on my mobile. I explained I had been in an accident and had no idea where I was. She told me to go to the nearest street corner and tell her the names of the streets. I did that and it turned out I was near the main train station about three and a half kilometres from where the accident occurred.
She came and got me and took me to the hospital, where they diagnosed concussion (duhh!), cleaned and bandaged my wounds, and kept me overnight under observation. When I returned to work and told colleagues what had happened, one of them told me he had seen me on my bicycle riding in the traffic and had not noticed anything unusual. Apparently I am capable of riding in traffic while unconscious. Or perhaps conscious but without any memory-retention ability. I could easily have ridden in front of a car and been killed. As with the first experience, if that had happened I would never have known.
I guess death was a more certain possible outcome for the South African experience. If my friend had not seen me on the bottom of the pool and got me out in time, I would have almost certainly died. This was a much more traumatic experience (after the event) than other “near-death” experiences where I was conscious and realized I was likely to die. I’ll write about them in a later post.
I recently read a blog post by Nathan Hohipua in which he argues that it is impossible to (truly) imagine our deaths, and that the only possible attitude towards death is one of anxiety. He claims that “The light of consciousness cannot really, truly imagine its own extinction” and concludes that “Anxiety is the only possible response to death because it’s just what it is to contemplate something that literally can’t be contemplated because it is the end of all possibility of contemplation.“
I think he is wrong in generalizing his own inability to imagine the state of being dead to others. In the waterslide accident, I truly feel that I came back from an experience identical to that of being dead. No memory, no awareness, no experience, nothing. If I had not come back, I would never have known it. That realization has been profoundly disturbing. But the state of being dead? I experienced “not being there” in any form and its nothing at all to be afraid off. You don’t exist, and there is nothing to experience the not existing. I may be missing something, but I don’t have any problem accepting that there will be a future point after which I simply don’t exist. Its exactly the same as before the point in time at which I started to exist (some time after conception). I have not existed for billions of years and I will also not exist for billions more.
The process of gradually losing function and experiencing pain and possibly loss of mental functioning, whether through ageing or illness, that is a completely different issue. And something that does worry me. I am working on accepting and letting go of the mental drama about it. And eventually when needed, do some contingency planning and prepare a living will. Nathan Hohipua says that if someone tells you they have completely accepted their death, they are deceiving themselves. That likely is true in some cases. And might be true if you are referring to the process leading up to the point of death. But completely untrue for me, if you are referring to the state of being dead. I’ve experienced it, and its nothing to be afraid of.
In two earlier posts about breathwork (here and here), I described my experiences with Wim Hof breathwork and transformational breathwork. More recently I have done a three-day holotropic breathwork retreat and a workshop on transformational breathwork, which gave me the chance to experience a range of breathing techniques.
A friend recommended I read Breath: the new science of a lost art, by James Nestor. Published in 2020, this book became a New York Times bestseller. It describes Nestor’s 10-year journey exploring various forms of breathwork and the scientific research about them.
The first half of the book examines breathing methods for improving health. Nestor focuses extensively on nose breathing versus mouth breathing and on various “under-breathing” techniques which are said to make dramatic differences to chronic lung conditions such as asthma and emphysema, as well as promoting general good health and increased endurance and athletic performance. Nestor spends some time discussing his experiment in solely mouth-breathing for two weeks (his nostrils were physically blocked for the duration) followed by two weeks of solely nose breathing. He taped his lips shut at night so he would not mouth-breath while asleep. He took extensive measurements of physiological indicators and other factors, such as time spent snoring. Mouth breathing resulted in substantially worse health and mental states, as well as higher blood pressure and heart rates. Nose breathing resulted in dramatic improvements. He also reviews a lot of research and ancient knowledge supporting these conclusions.
James Nestor having his nasal passages examined
This half of the book was fascinating, and I’ll certainly experiment with some of the techniques. Although he warned that breathing methods will not cure cancer or make an embolism go away, this part of the book still reminded me of books I’ve read where the author claims their diet, exercise, or whatever, will cure all your health problems and turn you into a high-functioning human.
Wim Hof, the Iceman
The second part of the book looked at breathing techniques which are more extreme and claimed to be radically transformative. These include various forms of breathwork which affect the autonomous nervous system and can improve immune system function and the ability to withstand extreme cold. Wim Hof breathwork is a well-known form of this and Nestor spends quite some time reviewing studies of it, and investigating the biological mechanisms involved. He does practice some Wim Hof breathwork with an instructor, but as far as I could tell, did not actually include cold exposure training. He much more briefly discusses holotropic breathwork and his discussions with Stan Grof and other holotropic breathwork instructors. He did one holotropic breathwork session early in his exploration of breathing methods and did not experience much at all. He is dismissive of other participants who had dramatic experiences, noting that their breathing did not appear much more intense than his and that their experience came on very quickly. He largely dismisses the effects of holotropic breathwork as psychosomatic (due to set or setting rather than the breathing technique).
I was disappointed in the inadequacy of his approach to understanding it. My experience is that the results of holotropic and other forms of breathwork is very dependent on your willingness to open to rather than resist the experience (yes, set is important). To a greater extent than in psychedelic drug trips, the holotropic breather is largely in control the intensity of the experience. In my first transformational breathing session, I held back from allowing the bodily energy and emotions full expression due to embarrassment, but later I found that I would very rapidly start to experience powerful emotions and bodily energy in a breathwork session. Nestor’s description struck me as that of someone who had held back in their first and only holotropic session.
A third type of breathwork covered in the second part of the book involves drastically increasing the concentration of carbon dioxide in the air breathed. Normal outdoor air concentration of CO2 is around 0.04% and carbon dioxide therapy involves breathing a mixture of 15-35% CO2 with normal air. Although blood oxygen levels do not change significantly, the very high concentration of CO2 induces an intense fear of not being able to take another breath and arises from chemoreceptors in the brainstem. It is a much more primitive and uncontrollable biological reaction than fear mediated by the amygdala. I recently met someone who told me he had purchased a cylinder of CO2 and was experimenting with breathing mixtures involving around 7% CO2. He claimed that this invoked a very intense fear of death which enabled him to break through to deep unconscious fears and address them. At the time I had not read this book and thought he was a nutcase. Nestor claims that this form of conscious breathwork (a much more intense version of breath-holding practice) allows the practitioner to develop much greater chemoreceptor flexibility and tolerance. In effect, it vaccinates the practitioner against excessive stress responses to events in their life. Hmm, its an extremely unpleasant experience, and I think I will pass.
James Nestor breathing high concentration of carbon dioxide
While I was disappointed at Nestor’s lack of interest in exploring holotropic and related forms of transformational breathwork, I did learn a lot and enjoyed reading the book overall. I can see why it was a bestseller in the pandemic period, when no doubt many people were stuck in lockdown with time to experiment. Anyway, I’m heading to the bathroom now to shave off my moustache so I can tape my mouth shut tonight.